
Blog
For most of my practice of coming alongside people in care or at the end of life, my harp has been the extension of me. It has traveled in ICUs, nursing homes, funerals, and celebrations of life. But for George, it couldn’t reach into the depths of his ears or into his soul for soothing, comforting, and connecting. George became profoundly deaf at the end of life. George, in his youth, was a very active and attractive young man with many skills athletically and also musically. Both he and his brother were incredible tenors in their church choirs from youth until their sixties. They sang duets and solos in church and with Gilbert and Sullivan Productions. It was actually there that George met the love of his life, Audrey, and they sang together. In my youth at church, George was often gowned in the choir garb, enjoying the music of the church and those “olde hymns”. Later, George’s father’s work as an assayer took him at the age of 16 to Jamaica, where he fell in love with the folk music of the isle. At home, he loved watching Don Messer’s Jubilee; country music was his soft spot. Often after dinner, he would start the turntable and listen to the crooning of the country and western storytellers. Aging, as they say, is not for the faint of heart. The loss of hearing was a huge adjustment for George, and the loss continued until even the hearing aids no longer worked. I would take Ruby, my little red harp, into the nursing home to play, and he would gently smile in his George way and shake his head that he heard nothing. This is where I became the student during the journey. George would bring out copies of his music, such as old hymns and lyrics of favourite love songs. These copies would be yellowed and delicately thin with age. He would begin to sing in his mellow tenor voice, and the memories flooded back. He shared the copies with fellow residences and staff. He would sing to them all. My job was to listen and take in his rich history of music that journaled the passages of his life. Our favourite haunt in the last nine years was Swiss Chalet, every Sunday evening. Often, our Jamaican staff would come out and sing to George. He really couldn’t catch the words the first couple of times, and then he would lip-read Diane’s words, “Come, Mr. Tally Man, Tally Me Banana,” and everyone at the table and surrounding tables would sing. George would randomly sing songs of the past during these dinners, remembering all the words as well as the moments these songs elicited. Then, the talk and connection went deep. His son, Peter, would take notes about all of these wonderful events of a man who lived a humble life well. Our portal into the life of George often came through old black-and-white photos, old hymn books, even old 78 records. He would smile, close his eyes, relax in his lazy boy, and the vocal music would begin. With the music came the stories of life traveling with his family, the depression, World War 2, meeting Audrey, raising his family, and connection with others through music. Even though he could no longer hear, he remembered and could still give the gift of song to others. The lesson is that music is so much more than sound; it is the connection, the stories, and the memories. We, as music care advocates, need not pass by someone who can’t hear as we may feel not useful, but to think beyond the physical sound into the memories of a song. The use of old pictures and hymn books helped us to enter into the past, as did the conversations cards of Music Care. Our job is one of connection and valuing the humanity of a soul. Music provides rich soil for connection. As our body ages and access to many things diminishes, we must still consider how to adapt our approach of using music to connect, through pictures, conversations, touch, and just being in space together sharing who we are. Shelley Neal is a special education teacher and program coordinator, therapeutic musician, and music care advocate in the Greater Toronto Area. Shelley uses music to deliver curriculum, support movement and language development and communication skills with non-verbal children. Her goal is to come alongside people and use music in whole person care.

There are moments in nursing that stay with us forever, and others that seem to pass by without much notice or fanfare. Many nurses, for example, vividly remember the excitement and nervous anticipation that accompanied their first job. In contrast, writing a first care plan rarely evokes the same intensity of emotion or lasting memory. Yet, care planning is a fundamental component of nursing practice. Effective care plans help the healthcare team communicate clearly, understand each member’s role, and collaborate in meeting the individualized needs of every resident. As a Registered Nurse, I have seen that personalized care can make a real difference in the lives of older adults. One simple but powerful example is planning music care. When music is intentionally added to a resident’s care plan, it becomes much more than entertainment. Music can be used as a therapeutic tool that improves comfort, connection, and quality of life. What makes music so valuable is that it is simple, easy to access, and adaptable to each person’s preferences. Music is at your finger tips with the use of Spotify, Amazon Music, YouTube, and other streaming services. In addition, programs like Music Care by Room 217 help healthcare teams excel in the safe and effective use of music in care. From a nursing perspective, music fits naturally into holistic care, which means caring for the whole person, not just their physical health. Nurses look at emotional, mental, social, and spiritual needs as well as physical symptoms. Music can support all of these areas. It can help reduce anxiety and agitation, encourage movement, improve mood, promote relaxation, and even lessen the feeling of pain. In long-term care, staff often support residents during vulnerable moments, such as personal care, transitions, or times of distress. Music can help these moments by creating calm and comfort. One resident experience clearly showed me how powerful music can be. This resident was living with dementia and had some communication deficits. As part of a quality improvement initiative at Glen Hill Terrac e, staff gathered more information about the resident’s musical preferences and created a personalized music-based care plan. The change was remarkable. During care, while this personalized musical list was playing, the resident started singing along with staff, engaging positively, and had enhanced verbal communication. Most importantly, music helped the resident reconnect with moments of joy. Quality care is about more than treating illness. It means supporting dignity, comfort, joy, and human connection. Music is a simple but powerful tool that reaches people in ways medicine alone cannot. When thoughtfully included in care plans, music becomes part of compassionate, person-centered approach to caring. Juanne George is the Director of Dementia Care at Glen Hill Terrace, a 160-bed Long-Term Care Home.

Several years ago, I met Brian*, a young adult who was living with stage 4 lung cancer. The highly aggressive disease had metastasized to multiple parts of his body, including his brain. In our lengthy conversations over many music therapy sessions at the hospital, I was struck by his focus on legacy. He told me he was constantly wondering if and how he would be remembered. At only 27 years old, he was at once youthful and existentially weighed down by the reality of the disease progression, eager to soak in as many experiences as he could while being mindful that his time was limited. As a music therapist, I often focus on “legacy work” through songwriting as a vehicle for creative self-expression but also as an offering to the patient’s family. The songs I write with patients who are receiving palliative and end of life care often represent that which holds meaning to them. We write songs for loved ones, about loved ones, about oneself, about hopes, dreams, regrets, ideas, and reflections. Sometimes the patient wants to infuse humour, other times the lyrics and chord progressions are pensive, even melancholic. However, the songs come together, they always serve as a form of legacy. Perhaps that is an intrinsic outcome of songwriting: it’s inherently representative of a point in time and can be revisited as a reflection of that moment, of that person, of that experience or relationship. In one of our music therapy sessions, I introduced the idea of songwriting to Brian, who immediately connected with the concept and told me he’d be thrilled to try it, though he wasn’t sure what he wanted to say or how the process would unfold. Together, over several weeks, he and I crafted lyrics, which he would later speak atop a chord progression we created. He told me he wanted the chords to feel “deep, painful, yet hopeful,” a contrast which he named as his own current reality, as he was balancing living while dying. I had heard of other music therapists recording patient heartbeats with a stethoscope and using the audio as a backing track of sorts, a rhythmic line that threaded through the song. Having just been generously gifted a digital stethoscope from a community organization, I knew in my own heart that Brian would be the perfect first patient for me to create a heartbeat recording with at the hospital. With a little help from my nursing colleague, we recorded Brian’s heartbeat, embedded the sounds into the track he and I had written and recorded, and a few days later, presented it to his family. Brian died several months later but his vitality remains embedded into the song he wrote, both in the music and lyrics but also in the acoustic representation of his life force: his heartbeat. Over the past several years, music therapists have been using heartbeat recordings as legacy work with patients and families in a number of settings including but not limited to oncology, pediatric intensive care units, and hospices. Last year, together with the Adolescent and Young Adult (AYA) Oncology Program at Princess Margaret Cancer Centre , the Music Therapy Program launched a “Heartbeat Recording for AYAs” research project where we will be writing songs with this patient population and researching the lived experience of the legacy work and heartbeat recording for these patients. We’re so thrilled to be able to carry on this work as a research endeavor and hopefully come to a richer understanding of the impact of this songwriting approach. When I reflect on the work Brian and I did together, I’d like to think he would be excited to see this type of legacy work expanded for adolescents and young adults. Perhaps his courage to be the first patient to trial this experience is part of his legacy, too, and I will be forever grateful. Dr. SarahRose Black PhD RP MTA is a certified music therapist and registered psychotherapist, specializing in palliative care and psychosocial oncology at the Princess Margaret Cancer Centre, and her private psychotherapy clinic (Whole Note Psychotherapy) in Toronto, Ontario. She is a pianist, vocalist, and music health educator, and has performed, taught, and presented on her clinical work and research across Canada.

Music is everywhere. It plays in the background of waiting rooms, fills quiet spaces, and is often added to care environments with good intentions. But music care is not just about playing music. The difference is intention. In music care, intention means using music with a clear purpose. It is not just about what is playing, but why it is being used, when it is introduced, and how it supports the moment. It is the difference between turning on any playlist and choosing the right piece of music for what is happening right now. This shift may seem small, but it changes how music functions in care. When music is used intentionally, it moves from background to something that actively supports the care process. A familiar song used at the same time each day can help signal routine. A slower tempo can support calm during moments of agitation. An upbeat rhythm can encourage movement and participation. In each case, the music is doing something. It is not just filling space. It is supporting care. At its core, intentional music care can be understood in three connected ways: Use: How music is used in the moment Design: How music is structured and selected to support care Performance: How music is expressed and adapted to suit different settings and care scenarios

With the Juno Awards taking place this past weekend, there has been a renewed focus on the role music plays in Canadian culture. It brings people together and creates shared moments. This same idea surfaced in a different context earlier last week. During the recent Ontario Long Term Care Association conference, a keynote from Mike Downie, Telling Our Story: The Power of Narrative to Inspire and Connect, reflected on the legacy of his brother, Gord Downie, and the impact of The Tragically Hip. One of the main insights of this reflection was a simple idea: music connects people. During the keynote, reflections shared from residents at Kensington Health offered a powerful reminder: Music is a common ground for community gathering It is not about what is lost, but what is still there Music that has meaning can bring us back, even if only for a moment Mike Downie also reflected on how the storyteller can become the story. This is a clear theme in the life of Gord Downie, who was known for storytelling through his lyrics and later became the story himself through his health journey. His later work, including Secret Path , also highlighted his advocacy for Indigenous communities and demonstrated how music can be used to share stories that might otherwise go unheard. In care environments, this idea shows up in different ways. Projects like The Green Bench create space for people to share their stories directly. Music can do something similar. It can bring forward identity, memory, and moments of self-expression, even when communication changes. These reflections may feel familiar to those who work in care environments. It may look like a resident quietly joining in with a familiar song, or a shared moment where a room shifts as music begins. Connection through music may appear as: A familiar song leading to singing or humming A moment of recognition seen in a glance or a smile A shift in the tone of the room when music is introduced These moments of connection are often described as spontaneous. However, they are not accidental. Music, when used intentionally, can support connection in everyday care. This might look like: Choosing music that is familiar and meaningful to the person Using music to support transitions or care routines Creating opportunities for shared listening or singing The legacy of Gord Downie reminds us that music has always brought people together. In care environments, through the intentional use of music, that same connection continues.
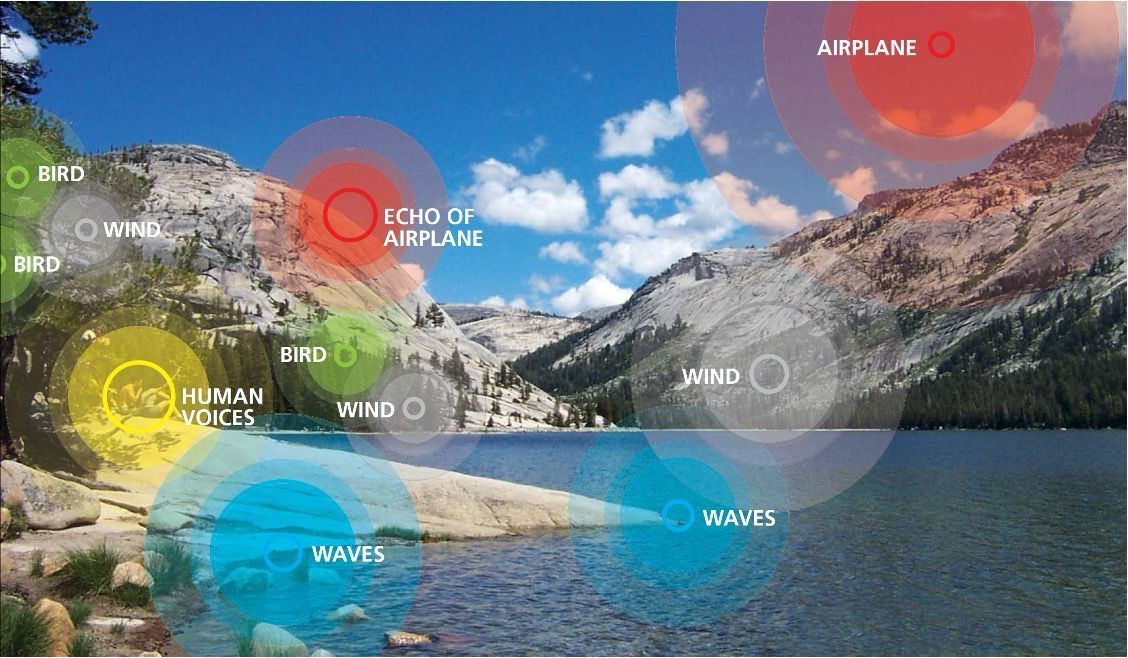
As I begin my role with MUSIC CARE by Room 217 , I am also beginning my own learning journey in music care. My background is in healthcare education and program development, with previous roles at Carpenter Hospice and the Princess Margaret Cancer Centre. In those settings, I had the opportunity to see music therapists at work and witness the impact that music can have in care environments. This week I began MUSIC CARE TRAINING Level 1 , the first level of standardized training offered through MUSIC CARE by Room 217. Even in the first part of the training, several ideas have already shifted how I think about music in care environments. One insight that stood out immediately came from the first session led by Dr. SarahRose Black , a music therapist, psychotherapist, and educator. She noted that music care is not limited to a specific professional role. A nurse manager who advocates for music care within their organization is also practicing music care. Creating the conditions where music can be used thoughtfully in care environments is itself a form of care practice. The same can be true for roles that people might not immediately associate with care practice. A receptionist who intentionally chooses calming music in a waiting area, or who notices how sound affects the mood of a space, can also influence the care environment in meaningful ways. In this sense, music care becomes less about a specific job title and more about an approach to how we shape the spaces where care happens. Another concept introduced in the training comes from music scholar Christopher Small , who described music not simply as a thing we listen to but as something we do. Small used the term “musicking” to describe the many ways people engage with music. This includes singing, listening, sharing songs, or creating musical moments together. In care settings, musicking can support connection, expression, and well-being. What struck me most, was a discussion about the soundscape of care environments. In many healthcare and long-term care settings, residents and patients have limited control over the sounds around them. Hallways can be busy. Alarms sound frequently. Televisions are often left on. Conversations carry across shared spaces. People naturally entrain to the rhythms and energy of their surroundings. Entrainment simply means that our bodies and emotions tend to sync with the patterns around us. When the environment is hectic or noisy, people may begin to feel unsettled or stressed. Dr. Black shared an example of an organization that, after completing the MUSIC CARE CERTIFY program, implemented an environmental sound policy to help regulate what influences the soundscape of their care environment. As she noted, “music can be a positive form of entrainment.” By intentionally shaping the sound environment, including the thoughtful use of music, care spaces can begin to shift from chaotic to supportive. In this context, music is not simply entertainment. It becomes part of how care environments are designed to support well-being. Music care is less about adding something new and more about bringing intention to something deeply human. It asks us to pay attention to our relationship with music and how it shapes the spaces where care happens.

Professionally, I have continued to develop my skills as a hand drum facilitator, moving beyond technique into a more intentional, care-focused approach. Incorporating Music Care strategies into drumming has transformed how sessions feel and function, allowing rhythm to become a tool for connection, engagement, and emotional expression. One of the most impactful strategies I’ve used is picking songs for care contexts during drumming facilitation. Choosing familiar and meaningful music creates instant buy-in and excitement. Some of the most joyful moments have come from drumming along to ABBA and AC/DC, songs selected by both team members and residents. These shared musical choices encouraged participation, helped everyone catch the rhythm more easily, and created an atmosphere of laughter, movement, and shared energy. The familiarity of the music allowed participants to feel confident and included, regardless of their musical experience. To support inclusive and adaptable sessions, I intentionally assembled a Music Care Kit tailored specifically for drumming facilitation. My kit includes a variety of drums, some smaller, some larger, and others with handles to support different hand grips. I also include drumsticks of varying weights to ensure adaptability for different strengths and abilities. A speaker is essential for song-based drumming, along with facilitator notes that help guide session flow. Additional instruments, such as chimes, allow me to introduce moments of calm during drum washes, while a jam drum block supports call-and-response interactions. Even my portable tote has become an essential part of the kit, allowing me to easily transport everything from one community to another. This flexibility ensures music care can meet people where they are. Music Care has also become a vital part of my personal self-care. I intentionally use music while driving to work as a way to decompress from the previous day or to prepare myself emotionally for a compassionate and grounded workday. This simple practice has helped me manage stress and transition more mindfully between personal life and professional responsibilities. Beyond daily routines, music now shapes how I experience the world. As part of my personal Music Care Plan, every vacation I take includes music as a way of learning about culture, history, and identity. In Norway, I attended a midnight concert in a local church in Tromsø and sang along with an Indigenous Sámi man who shared a song about his grandmother. In Poland, I experienced a Jewish Kazimierz performance featuring violin, singer, and accordion. In Ireland, I listened to harp and flute music at the base of the Rock of Cashel and played the drums at the Ireland Rock and Roll Museum. My travels also included attending Mozart, Strauss, and Beethoven concerts in Vienna, visiting Mozart’s birthplace in Salzburg, and participating in the Silent Night Chapel service on December 24. Each experience reinforced how music transcends language and creates a sense of belonging across cultures. Looking ahead, my journey with music continues to evolve. During my hand drum facilitation course, I unexpectedly fell in love with the didgeridoo. The low tones and full-body vibration felt deeply soothing and grounding. Quietly, I’ve signed up to learn how to play. This instrument requires internal and circular breathing, something I find challenging due to ongoing lung issues, but I see this as an opportunity rather than a limitation. Learning the didgeridoo may support Motor and Respiratory Exercises (OMREX) ® , a core Neurologic Music Therapy technique that uses singing and wind instruments to build respiratory strength and control. Through diaphragmatic breathing, increased expiratory pressure, and improved breath control, this practice has the potential to benefit both my personal health and my future work in care settings. Music Care has reshaped how I drum, how I travel, how I breathe, and how I care for others and for myself. What began as skill development has become a way of moving through the world with greater intention, curiosity, and connection.

A year goes by, time ticks on, we grow, we further our missions in life. This year was the year of music growth for me as a human. What does it mean to truly care for your fellow human and to use music as a catalyst to care for them? I garnered a lot of ways to do this in a year. What is the main thing I learned? Listening. What truly is the art of listening? I focused heavily on my 10 domains of care. The one I honed in on the most was environmental sound. The environment impacts us all, it’s our scope. The little things count, a movement. It can be a rhapsody, it can be fingernails on a chalk board. I focused on rhapsody and said hello to chalk board screeches. How could I make sounds more pleasant? I adjusted volumes to devices, tones, pitches. I created musical soundscapes that fit the unique quality of the human condition within our realm. I listened with quenches or smiles, I aimed for relieved looks, looks that said, “this sounds right.” I chose sounds that spoke to the tribe. When I worked one on one, I spoke to the spirit of the one. I’m listening to Bob Seger writing this and his song, “Against the Wind.” That’s what I did this year; I ran against the wind. I tackled an inevitable, sounds. Sound should speak to us all, not turn off our volume. I also learned how to help, not only myself cope with unpleasant sounds, but my folks I care for too. The answer? It lies in the acceptance. Call it out- admit it’s way of making you feel. Feel, hear, react, adapt. So, this year as I ran against the wind? The wind began to become a song instead of a gush. It now is more of an orchestra at our facility. Each little hiss, buzz, ring, ding, ting or veritable element of sound is something part of an accepted orchestra. Each or us tuned into our humanness here, in our domain. I also launched our own record label. It’s called Gentog Records, named after our mission. Generations together. We launched our first single to major distributors, it is called, “New Beginnings.” It is music written and inspired by humans dealing with neurodegenerative disorders with me as their Sherpa. It represents a big no to what we call “disease”. It shows that humanity and dignity exist, despite it all; the human spirit is the definition. The label is two-fold. 1) To offer ownership and authorship as creators over their sounds and over their feelings and stories. 2) Generate income for the non-profit we have Gentog Community Services. It’s been a year, one of triumph and failure. Still here we are, perhaps still running against the wind. But, bring on the wind! Embrace its orchestral movement. I know one thing for sure, I’m more in love with sound and humanity. And that, that sounds lovely.

As a psychologist and a researcher, I spend my days exploring the incredible benefits arts engagement can bring to the health and well-being of individuals across the lifespan. A particular focus of my work is on music, be it group singing in choirs, intergenerational music therapy that connects young children from the community with residents of long-term care homes, virtual opportunities for families to sing together from a distance, or high-quality concerts provided by professional musicians. Given my background, you’re probably wondering how I ended up leading a holiday sing-along with Toronto Mayor Olivia Chow in November… My current role is the perfect match for my longstanding interest in the arts. My love of music began at an early age. As I was the only niece living close by, I was my aunt’s regular “plus 1” for all sorts of musical performances coming through Montreal’s Place des Arts and Bell Centre. Growing up singing in choirs at church and in high school led to performances with the Hart House Singers when I moved to Toronto for graduate school. Over the last few years, my singing has been more commonly directed to an audience of two small children (and a cat), and I’ve harnessed my love of group singing into my research: I am currently involved with the SingWell project, an initiative out of Toronto Metropolitan University that examines physiological and quality of life benefits of group singing for a variety of populations, including individuals living with hearing loss, Parkinson’s disease, and dementia. So imagine my surprise and delight when I recently had a powerful reminder of the personal joy of group singing. One chilly day in November, I had the opportunity to walk in my local Santa Claus parade with the Mayor of Toronto. As we neared the end of the parade route, there was a bend in the road where our group decided to set up and play some holiday tunes. Unfortunately, it seemed as though the sound system was out of order, and Mayor Chow turned to the group and asked “who likes to sing”? I sprang to respond, flung up my hand, and was immediately brought to the front of our crowd and found myself- unexpectedly and delightedly- leading an extremely enthusiastic and joyful choir on a street corner just blocks from my home! We sang for about 15 minutes, cycling through a repertoire of tried and true holiday favourites, sometimes stumbling over the words, sometimes getting an assist from people passing by! Folks who were completing their own parade journey, joined in, sang along, shouted encouragement, smiled and waving as they passed. While singing, my inner scientist couldn't help but wonder- were my cortisol levels decreasing? Maybe my oxytocin, the human bonding hormone, was shooting through the roof! This unique opportunity was the perfect representation of so much of the work I have been doing for many years. Seeing so many faces breaking into smile (and so many people breaking into song!) was a keen reminder of the power of music to connect us, and emphasized the important work that the room 217 team does every single day.
